
Prostate-Specifc Antigen Modulatory Effect of a Fermented Soy Supplement for Patients with an Elevated Risk of Prostate Cancer
2021-02-24
Abstract
Objective: To investigate the efficacy of a 6-month fermented soy supplement (equol-containing), measured by prostate-specific antigen (PSA) stabilization or PSA decrease from baseline (PSA modulatory effect) in men with an elevated risk of prostate cancer (PCa), with a WHO performance 0-2 and a follow-up of 12 months. Methods: The patient population consisted of men with an elevated risk of PCa and a prior negative prostate biopsy within 1 year from starting therapy. Serum PSA values were recorded at inclusion (iPSA), at 6 months (1PSA), and optionally at 12 months (2PSA). Statistical analysis was carried out using the Wilcoxon rank sum test (p < 0.05). Results: In total, 137 men used fermented soy for any prostatic reason. After inclusion criteria for an elevated risk of PCa and a prior negative prostate biopsy, we selected 58 patients. Among these, there was a significant PSA modulatory effect (iPSA-1PSA, p = 0.003). This modulatory effect was more strongly evident in the subgroup of patients with an elevated iPSA (≥ 4 ng/ml) (n = 33, iPSA-1PSA, p = 0.003, iPSA-2PSA, p = 0.002). Conclusions: We demonstrated a significant PSA modulatory effect of a 6-month fermented soy supplement in men with an elevated risk of PCa and a prior negative prostate biopsy. This positive effect is currently being investigated in a prospective study. Further evaluation of the role of fermented soy supplements is warranted in a preventive and therapeutic setting of men at an elevated risk of PCa.
© 2020 The Author(s) Published by S. Karger AG, Basel
https://www.karger.com/Article/Fulltext/499246
Results
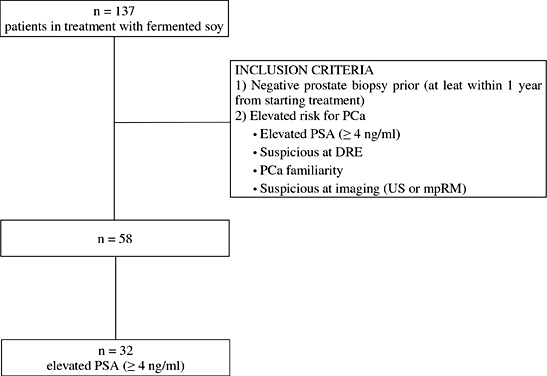
In total, 137 men used fermented soy for any prostatic reason. After inclusion criteria for an elevated risk of PCa and a prior negative prostate biopsy, we selected 58 patients. Their median age was 68 years (IQR: 58-73 years). Median follow-up was 11 months. Descriptive statistics are presented in Table 1.
Table 1
Descriptive statistics for patients treated with a fermented soy supplement between November 2013 and April 2016 at a single center
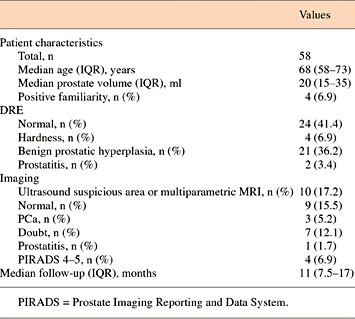
Table 2 shows the statistical significance (Wilcoxon rank sum test) of the PSA measured at the first control (iPSA-1PSA) and PSA measured at the second control (iPSA-2PSA) after fermented soy supplementation compared with the initial PSA at inclusion. For the subgroup of patients with an elevated PSA, the statistical significance of the 2PSA compared to the 1PSA (1PSA-2PSA) is also reported.
Table 2
Wilcoxon rank sum test for analyzing the PSA modulatory effect of a 6-month fermented soy supplement in patients with elevated risk of PCa (p < 0.05)
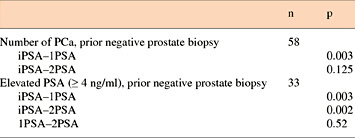
The 1PSA modulatory effect compared with the initial PSA values at inclusion reached statistical significance in the study group of patients with an elevated risk of PCa and a prior negative prostate biopsy (n = 58) (iP-SA-1PSA, p = 0.003) (Fig. 2). The 1PSA and 2PSA modulatory effect compared with the initial PSA values at inclusion reached statistical significance in the subgroup of patients with an elevated PSA (n = 33) (iPSA-1PSA, p = 0.003, iPSA-2PSA, p = 0.002) (Fig. 3).The PSA modulatory effect of the fermented soy supplement was more strongly evident in the subgroup of patients with an elevated iPSA.
Fig. 2
PSA modulatory effect of a fermented soy supplement in patients with an elevated risk of PCa and a prior negative prostate biopsy (n = 58). **The difference between iPSA and 1PSA was statistically significant (iPSA-1PSA, p = 0.003).
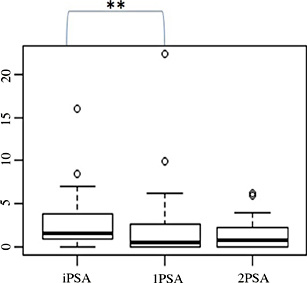
Fig. 3
PSA modulatory effect of a fermented soy supplement in patients with an elevated risk of PCa, a prior negative prostate biopsy and elevated PSA (≥ 4 ng/ml) (n=32). **The difference between iPSA-1PSA and iPSA-2PSA was statistically significant (iPSA-1PSA, p = 0.003; iPSA-2PSA, p=0.002).
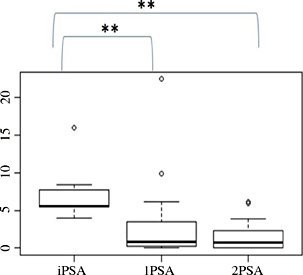
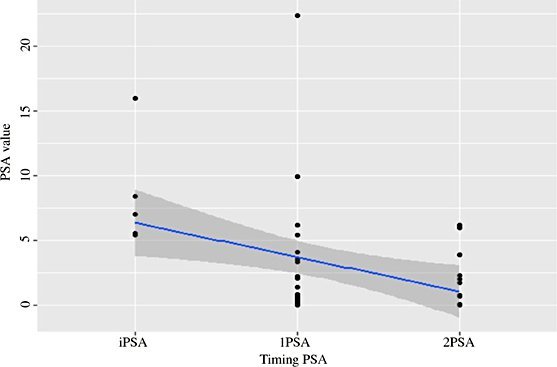
Figure 4 and 5 present the decrease of the PSA value during consumption of the fermented soy supplement in the study group (n = 58) and in the subgroup (n = 33), respectively.
Fig. 4
Decrease of the PSA value during consumption of the fermented soy supplement in patients with an elevated risk of PCa and a prior negative prostate biopsy (n = 58).
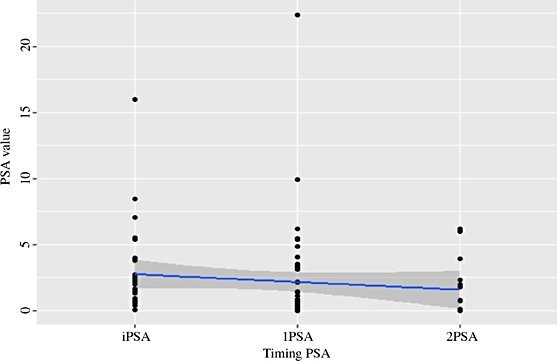
Fig. 5
Decrease of the PSA value during consumption of the fermented soy supplement in patients with an elevated risk of PCa, a prior negative prostate biopsy and elevated PSA (≥ 4 ng/ml) (n = 32).
Next
Categories
Recent posts